
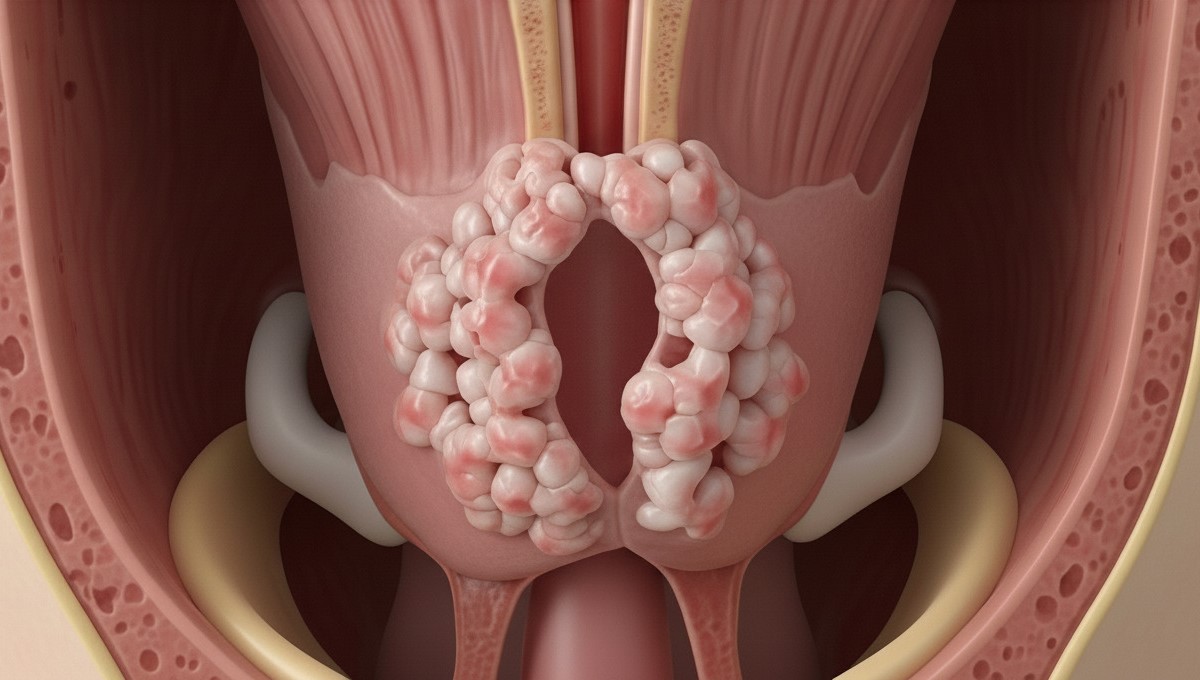
Laryngeal papillomatosis, also known as recurrent respiratory papillomatosis (RRP), is a condition where benign (non-cancerous) tumours called papillomas grow in the airways, particularly the larynx (voice box). These wart-like growths are caused by human papillomavirus (HPV) infection, specifically HPV types 6 and 11. The condition affects both children and adults, though the presentation and progression differ between age groups. The papillomas tend to recur even after removal, making this a chronic condition that requires long-term management and regular monitoring.
Laryngeal Papillomatosis in Singapore
Living with laryngeal papillomatosis can impact voice, breathing, and quality of life. This condition causes benign growths in the throat and the voice box, leading to hoarseness, breathing difficulties, and changes in voice. At our Singapore clinic, our ENT Specialist provides laryngeal papillomatosis treatment using modern techniques to manage symptoms and aim to preserve voice function. While this condition requires ongoing management, contemporary treatment approaches can help control growths and support quality of life. Individual results and treatment outcomes may vary.

Dr Gan Eng Cern
MBBS
MRCS (Edin)
mmed (orl)
FAMS
What is Laryngeal Papillomatosis?
Types of Laryngeal Papillomatosis
- Juvenile-Onset RRP (JORRP): Juvenile-onset laryngeal papillomatosis typically appears before age 12. This form may be associated with more frequent recurrences and growth of papillomas. Children with JORRP may require multiple surgical interventions throughout childhood. The condition can result from vertical transmission during childbirth from mothers with genital HPV infection.
- Adult-Onset RRP (AORRP): Adult-onset laryngeal papillomatosis generally appears in adulthood. This form may progress differently from the juvenile type and can have varying intervals between recurrences. Adult cases are thought to result from either reactivation of latent virus or new HPV exposure. Some adults may experience spontaneous remission, though this is unpredictable.
- Aggressive vs Non-Aggressive Disease: Regardless of the age of onset, laryngeal papillomatosis can be classified by its clinical behaviour. Aggressive disease may involve frequent recurrences, rapid regrowth, and potential spread beyond the larynx. Non-aggressive disease may show slower growth, fewer recurrences, and different treatment response patterns.
Causes & Risk Factors
Causes
The primary cause of laryngeal papillomatosis is infection with human papillomavirus (HPV), particularly types 6 and 11. These HPV types are considered low-risk for cancer but have an affinity for respiratory epithelium. The virus causes abnormal cell growth in the larynx, leading to papilloma formation. Not everyone exposed to HPV develops papillomatosis, suggesting that individual immune response may play a role.
Risk Factors
- Maternal HPV infection: Children born to mothers with genital warts may have an increased risk
- Immunosuppression: Weakened immune system from medications or medical conditions
- First-born status: First-born children may have a higher risk of juvenile-onset disease
- Vaginal delivery: May present a higher risk compared to caesarean section in mothers with active HPV
- Young maternal age: Younger mothers at delivery may have increased transmission risk
- Multiple sexual partners: May be associated with adult-onset disease
- Gastro-oesophageal reflux: May contribute to disease severity and recurrence
- Smoking: Can worsen disease progression in adults
- Previous intubation: Trauma to laryngeal tissues may facilitate viral infection
Signs & Symptoms
Mild Symptoms
- Progressive hoarseness lasting more than 2 weeks
- Voice fatigue after minimal talking
- Breathy or raspy voice quality
- Difficulty projecting voice
- Throat clearing or mild chronic cough
- Sensation of something in the throat
Moderate Symptoms
- Significant voice changes or complete voice loss
- Noisy breathing (stridor) during exertion
- Difficulty swallowing or choking sensation
- Recurrent respiratory infections
- Exercise intolerance due to breathing difficulty
- Voice breaks during conversation
Severe Symptoms
- Stridor at rest indicating airway obstruction
- Severe breathing difficulty or respiratory distress
- Cyanosis (blue discolouration) from poor oxygenation
- Complete airway obstruction requiring emergency intervention
- Failure to thrive in children
- Sleep apnoea or interrupted sleep from breathing problems
Symptoms may develop gradually over time. In children, voice changes are often among the first signs, whereas in adults, progressive hoarseness may be the first sign. The severity of symptoms can relate to the size and location of papillomas.
Experiencing these symptoms?
Consider consulting with an ENT specialist for proper evaluation and management.

When to See an ENT Specialist
Seek immediate medical attention if you experience stridor (noisy breathing), severe breathing difficulty, or any signs of airway obstruction. These symptoms indicate significant airway narrowing requiring urgent evaluation. Schedule a consultation if hoarseness persists beyond two weeks, especially if accompanied by breathing changes or swallowing difficulties. Parents should bring children with persistent voice changes or noisy breathing for assessment.
During your consultation, an ENT specialist typically performs a comprehensive throat examination, including flexible laryngoscopy. This procedure involves passing a thin, flexible camera through the nose to visualise the larynx directly. The examination aims to visualise any papillomas. Intervention may help prevent progression to airway compromise and aims to support voice preservation. Regular monitoring after diagnosis can help detect recurrences.

Diagnosis & Testing Methods
Accurate diagnosis of laryngeal papillomatosis requires direct visualisation and often tissue confirmation. An ENT specialist employs several diagnostic approaches to evaluate the extent of disease and plan appropriate treatment.
Flexible laryngoscopy is the primary diagnostic tool, allowing real-time visualisation of the larynx in the clinic setting. This procedure requires no special preparation. The examination may reveal characteristic warty, grape-like lesions on the vocal cords or surrounding structures. Video documentation can help track disease progression over time.
Direct laryngoscopy under general anaesthesia provides a detailed examination. This procedure allows for complete airway assessment, tissue biopsy, and simultaneous treatment. A biopsy confirms the diagnosis and rules out malignancy, particularly important in adult patients. HPV typing may be performed to identify the specific viral subtype, which can influence prognosis.
Imaging studies, including CT or MRI scans, assess disease extent in severe cases. These studies identify subglottic or tracheal involvement not visible on routine examination. Pulmonary function tests objectively evaluate the degree of airway obstruction.
Treatment Options Overview
Surgical Management
- Microlaryngoscopy with CO2 Laser: CO2 laser ablation is a recognised approach for removing laryngeal papillomas. This technique uses focused laser energy to vaporise papillomas whilst aiming to minimise damage to surrounding healthy tissue. The procedure requires general anaesthesia. Patients may return home the same day. The CO2 laser offers precision, which can help reduce the risk of scarring and preserve voice quality.
- Microdebrider Excision: The powered microdebrider offers an alternative to laser surgery, using a rotating blade to remove papillomas. This technique provides visualisation by continuously suctioning blood and debris. Some surgeons use this method for bulky disease, as it allows debulking. The procedure duration and recovery are similar to laser surgery.
- Coblation Technology: Coblation uses radiofrequency energy to dissolve papillomas at relatively low temperatures. This technique may reduce thermal damage to surrounding tissues compared to traditional methods. The technology can be helpful for papillomas in challenging locations. Recovery time and voice outcomes are comparable to other surgical procedures.
Medical Management
- Adjuvant Cidofovir Injection: Intralesional cidofovir injection during surgery may extend the interval between procedures. This antiviral medication is injected directly into papilloma sites after surgical removal. Whilst not curative, cidofovir may reduce the frequency of recurrences in selected patients. Regular monitoring for potential side effects is necessary.
- Systemic Bevacizumab: Bevacizumab, an anti-angiogenic agent, may be considered for aggressive disease. This medication inhibits the blood vessel formation that papillomas need to grow. Treatment involves intravenous infusions. Some patients may experience disease control. Close monitoring for side effects, including hypertension and proteinuria, is required.
- Interferon Therapy: Interferon alpha was previously used as adjuvant therapy but has largely been replaced by newer agents. This immunomodulator can slow papilloma growth but requires subcutaneous injections. Side effects, including flu-like symptoms, may limit its use. Current practice reserves interferon for cases unresponsive to other treatments.
- Proton Pump Inhibitors: Managing gastro-oesophageal reflux with proton pump inhibitors may improve outcomes. These medications reduce acid exposure to the larynx, potentially decreasing the risk of papilloma recurrence. Treatment involves daily oral medication. This adjuvant approach may be critical in patients with documented reflux disease.
Emerging Therapies
- HPV Vaccination: Whilst not a treatment for existing disease, HPV vaccination may influence disease course. Some studies suggest vaccination might reduce recurrence rates, though evidence remains limited. The quadrivalent or nine-valent HPV vaccines target the causative viral types. Vaccination is considered safe in patients with existing papillomatosis.
- Photodynamic Therapy: Photodynamic therapy combines a photosensitising agent with specific wavelength light to destroy papillomas. This experimental approach may help reduce recurrence rates. Treatment requires special equipment not widely available. Further research is needed to establish its role in routine management.
Every patient’s condition is unique.
Our ENT Specialist can assess your specific situation and recommend the most suitable treatment.
Complications if Left Untreated
Untreated laryngeal papillomatosis may progressively worsen, potentially leading to airway obstruction. Papillomas can continue to grow and multiply, gradually narrowing the airway until breathing becomes compromised. An emergency tracheostomy may be necessary if obstruction occurs. Children may be particularly vulnerable as their smaller airways can obstruct more readily.
Voice quality may deteriorate without treatment as papillomas can affect vocal cord structure. Chronic inflammation and repeated trauma from coughing may cause scarring. Some patients may develop voice changes that could require alternative communication methods. Professional singers or speakers may experience career impacts without timely intervention.
Disease may spread beyond the larynx in some untreated cases. Papillomas can extend into the trachea and bronchi and, in some cases, into the lungs. Pulmonary involvement may carry a more challenging prognosis with limited treatment options. Malignant transformation, whilst uncommon, may increase with disease duration and smoking exposure. Quality of life may deteriorate due to breathing difficulties, voice changes, and social impacts.
Prevention
While complete prevention of laryngeal papillomatosis is not always possible, several measures may help reduce risk. HPV vaccination before sexual activity can provide protection against the causative viral types. The vaccine is recommended for both males and females in Singapore, starting at age 9-12. Vaccination may also benefit sexual partners of affected individuals.
Pregnant women with genital HPV should discuss delivery options with their obstetrician. While caesarean section may reduce transmission risk, it does not eliminate it entirely. Children born to HPV-positive mothers typically do not develop papillomatosis. Regular prenatal care allows for appropriate planning and counselling.
Managing gastro-oesophageal reflux with dietary modifications and medications may help prevent worsening of the disease. Avoiding smoking and secondhand smoke exposure may reduce progression risk and potential malignant transformation. Maintaining good general health and immune function through proper nutrition and stress management may help control viral activity. Safe sexual practices may reduce adult HPV exposure, though the relationship to laryngeal disease remains unclear.
For Singaporeans & Singapore Permanent Residents
Medisave & Insurance Shield Plan approved
Your ENT procedure may be eligible for Medisave claims, with the claimable amount varying based on the procedure’s complexity. For additional options, including the use of your insurance or Integrated Shield Plan, reach out to our friendly clinic staff today for assistance.







Frequently Asked Questions (FAQ)
Is laryngeal papillomatosis contagious to family members?
Laryngeal papillomatosis is not contagious through casual contact, talking, or sharing utensils. The HPV virus requires direct contact with infected tissue for transmission. Family members are not at risk from routine interaction with affected individuals. However, the HPV types causing laryngeal papillomatosis can be transmitted sexually between partners. Children typically acquire the virus during birth from mothers with genital HPV infection, not through later contact.
How many surgeries will I need for laryngeal papillomatosis?
The number of surgeries varies significantly between patients and cannot be predicted at diagnosis. Some patients may require procedures annually, while more active cases may need surgery more frequently. Children generally require more frequent interventions than adults. Additional medical treatments may extend the interval between surgeries. Your ENT specialist can monitor disease activity closely and recommend surgery based on symptoms and examination findings rather than fixed schedules.
Can laryngeal papillomatosis turn into cancer?
Malignant transformation is rare. Risk factors include smoking, radiation exposure, and infection with certain HPV types. Regular monitoring allows early detection of any concerning changes. Suspicious lesions are biopsied promptly for evaluation. Most patients with laryngeal papillomatosis do not develop cancer. Your ENT specialist performs thorough examinations at each visit to identify any atypical features requiring further investigation.
Will my voice return to normal after treatment?
Voice improvement after treatment depends on the extent and vocal cord condition before surgery. Many patients may experience improvement in their voice, though complete normalisation may not occur in severe cases. Modern surgical techniques aim to preserve the voice while removing papillomas. Voice therapy after surgery may optimise outcomes. Early treatment before extensive scarring improves the likelihood of voice recovery. Speech therapists can work with patients to maximise voice function.
Can HPV vaccination help if I already have laryngeal papillomatosis?
HPV vaccination’s role in existing disease remains under investigation. Some studies suggest that vaccination might reduce the frequency or severity of recurrences, though the evidence is limited. The vaccine is safe for patients with papillomatosis and may provide protection against other HPV types. Vaccination does not replace standard surgical and medical treatments. Your ENT specialist can discuss whether vaccination might benefit your specific situation based on current evidence.
Is laryngeal papillomatosis hereditary?
Laryngeal papillomatosis is not inherited genetically. The condition results from HPV infection, not genetic transmission. However, individual immune response to HPV, which may have genetic components, influences disease development. Children of affected parents are not at increased risk unless exposed to HPV. Family members do not require screening unless they develop symptoms. Genetic counselling is not necessary for this condition.
What lifestyle changes help manage laryngeal papillomatosis?
Several lifestyle modifications may help with disease management and voice preservation. Staying well-hydrated can help keep vocal cords lubricated and may reduce irritation. Avoiding voice strain through proper voice use techniques can help prevent additional trauma. Managing acid reflux through dietary changes and medications may reduce laryngeal irritation. Stopping smoking is essential as it can worsen the disease and increase cancer risk. Regular exercise and stress management may support immune function. Healthcare professionals can provide comprehensive guidance on lifestyle considerations.
Can children with laryngeal papillomatosis participate in sports?
Most children with well-controlled papillomatosis can participate in age-appropriate activities. Exercise tolerance depends on airway patency and breathing capacity. Contact sports require careful consideration if a tracheostomy is present. Swimming may need to be modified based on airway status. Regular monitoring helps ensure safe participation levels. Your ENT specialist can provide specific activity guidelines based on each child’s disease severity and treatment status.
Conclusion
Laryngeal papillomatosis presents ongoing challenges, but modern treatment approaches can help manage the disease and preserve quality of life. By combining contemporary surgical techniques with adjuvant medical therapies, patients may achieve improved voice function and breathing. While the condition requires long-term management, individuals can lead productive, everyday lives with appropriate care. Early diagnosis and treatment can help prevent complications and may optimise outcomes. Our ENT Specialist combines experience with current treatment modalities to provide comprehensive papillomatosis care tailored to each patient’s needs.
Take the First Step Towards Better Health
Living with laryngeal papillomatosis can be challenging, but you don’t have to face it alone. Our ENT Specialist has experience diagnosing and treating laryngeal papillomatosis using current evidence-based approaches.

Dr Gan Eng Cern
MBBS
MRCS (Edin)
mmed (orl)
FAMS
With over 15 years of experience, Dr Gan specialises in the comprehensive management of a broad range of conditions related to the ear, nose and throat (ENT), and head and neck.
Dr. Gan has contributed to the academic field as a Senior Clinical Lecturer at the Yong Loo Lin School of Medicine, National University of Singapore. He underwent his subspecialty training in Rhinology (Nose & Sinus conditions) and Endoscopic Skull Base Surgery at the renowned St Paul’s Sinus Center, part of the University of British Columbia in Vancouver, Canada. He is recognised for his extensive research work, with numerous contributions to reputable international ENT journals. Dr Gan is also highly sought after as a speaker and has shared his surgical knowledge as a surgical dissection teacher at various prominent ENT conferences and courses.
- 2020 – Reader’s Choice Gold Award for Best ENT Specialist (Expat Living Singapore)
- 2016 – Best Educator Award (Eastern Health Alliance)
- 2016 – “Wow” Award (Patient Compliment)
- 2014 – Eastern Health Alliance Caring Award – Silver
- 2014 – 19th Yahya Cohen Memorial Lectureship (awarded by the College of Surgeons, Academy of Medicine Singapore for best scientific surgical paper)
- 2012 – Human Manpower Development Award (Ministry of Health, Singapore)
- 2007 – Singhealth Best Doctor Award
Qualifications
- MBBS – Bachelor of Science, Bachelor of Medicine, Bachelor of Surgery (University of New South Wales, Sydney, Australia)
- MRCS (Edin) – Member of the Royal College of Surgeons Edinburgh, United Kingdom
- MMed (ORL) – Master of Medicine in ENT (National University of Singapore)
- FAMS – Fellow of the Academy of Medicine Singapore

Make an Enquiry
Fill up the form and our friendly clinic staff will get back to you promptly.
Our Location
A Specialist Clinic for Sinus, Snoring & ENT
38 Irrawaddy Road #08-45
Mount Elizabeth Novena Hospital
Singapore 329563
Mon – Fri: 9:00 am – 5:00 pm
Sat: 8:30 am – 12:00 pm